 Central General Practice
Central General Practice
 Repulse Bay
Repulse Bay
 Clearwater Bay
Clearwater Bay
 BodyWorX Clinic
BodyWorX Clinic
 Central Specialist Clinic
Central Specialist Clinic
 MindWorX Clinic
MindWorX Clinic
 Family Clinic
Family Clinic
 OT&P Annerley Midwives Clinic
OT&P Annerley Midwives Clinic
 WellWorX Clinic
WellWorX Clinic


Written By: Dr David Owens
Over the course of the pandemic, I have written a series of articles analysing the Hong Kong Covid response. As China begins to shift away from the strategy of ‘dynamic zero Covid’, this article considers how lessons learned from the different strategies in Hong Kong and Singapore can best be applied when considering the current challenges facing the mainland.
A Pandemic of Two Halves
The Covid pandemic can be considered in the context of two distinct phases, pre and post-availability of vaccines. Early in the pandemic, before the development of vaccines, there were broadly two strategies employed internationally.
-
- Elimination, that is zero Covid. The focus was on case identification and control. This involved testing to identify cases, tracing the contacts of these cases and isolating both infected individuals and their contacts to prevent community spread. Border quarantine was used to prevent the importation of infections.
- Suppress and lift. Public health measures were increased or reduced depending upon the rise and fall of infective waves in the population. In this context, public health restrictions were predominantly designed to take the pressure off health systems. This strategy was employed with varying degrees of success in different countries.
There is good evidence that elimination was the most effective strategy in the first phase of the pandemic. Mortality rates, disruption to daily life and economic damage were all significantly lower in countries which eliminated before the availability of vaccines[1].
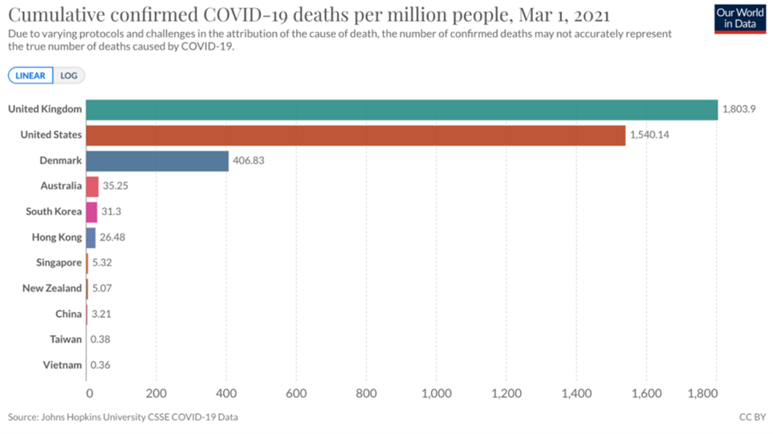
Fig 1. By the time vaccines were available the elimination countries (Australia down) had significantly lower mortality rates. The US, UK and Denmark show significant differences between countries that pursued different mitigation strategies.
Second Half: Politics and the Dilemma of the Pivot
By mid to late 2021 it was obvious that regardless of the political goals, the science suggested that permanent elimination of the SARS-COV 2 virus would be impossible. The evidence of transmission dynamics in addition to a better understanding of evolving mutations and vaccine-induced and innate immunity suggested that eventually a strategic pivot to living with Covid would be inevitable. The questions became those of the timing of the transition, whether the eventual pivot would be planned or forced and the optimal mitigation strategies needed to protect health systems during the transition.
China has a huge population and whilst health systems in urban centres are rapidly evolving, rural health infrastructure remains vulnerable. Chinese public health experts had also until recently expressed concerns about the population impact of Long Covid. In this context elimination was a valid strategy until high levels of vaccination, drug procurement and preparation of the health system had been achieved.
At its most basic continuation of a successful elimination strategy requires three components:
-
- Testing to identify cases
- Tracing to identify contacts
- Isolation of contacts, to identify secondary infections and break transmission chains
This process breaks down when capacity at any point in the chain is exceeded. Unlike other countries, China built enormous capacity in all areas of testing, tracing and isolation. Factors within the political system allowed for rapid and high-volume lockdowns. This was facilitated by community organisations at the district level and the widespread use of digital technology to identify potential contacts. President Xi made Zero Covid a signature policy and China was very successful in protecting the population throughout the first phase of the pandemic. There was a high degree of public trust in the Zero Covid strategy until at least early 2022. Until very recently, the political narrative within China was that 'dynamic zero Covid' was for the long-term and not a transitional strategy.
Unlike China, Hong Kong never developed the structural capacity to continue elimination. In an article in June 2021, I explained why Zero Covid was not a sustainable strategy for Hong Kong.
'Although desirable, zero Covid is not a viable long term solution to the pandemic. The evidence would suggest that countries which excelled in implementing zero Covid as a short term policy, now need to focus on boosting vaccine uptake, and therefore immunity in populations.'
'Zero Covid has been a very successful strategy for Hong Kong but it was always a waypoint on the journey to population immunity via vaccination. Increasing vaccine uptake involves not only education but the explicit recognition that absolute risk can never be eliminated, it can only be mitigated.'
'High vaccine coverage, especially for the vulnerable and a transition to living with Covid is ultimately the only viable long term solution'.
In an article in October 2021, I described the public health priorities for Hong Kong.
'In the case of Covid the following are the public health priorities for Hong Kong, in order:
1. Increasing vaccine uptake in the old and vulnerable
2. Increasing vaccine uptake in the old and vulnerable
3. Increasing vaccine uptake in the old and vulnerable'
By this time, it was very clear that Hong Kong did not have the infrastructure or capacity to pursue the same strategy as China.
‘Notwithstanding the clear strategic and commercial value of the mainland border, the science suggested that by late 2021, if the only goal had been a focus on population health, then the best public-health strategy for Hong Kong was to maximise vaccination rates from the vulnerable down with the best available vaccines and use the same strategy as Singapore.’
Second Half: Hong Kong and Singapore
We now have irrefutable evidence that the optimal strategy for the second phase was to achieve high levels of vaccination from the most vulnerable down. The demographic and geographic similarities and differences between the international business and travel hubs of Hong Kong and Singapore are well recognised. Both locations pursued similar strategies early and both had early access to the same vaccines. The comparison of outcomes between Hong Kong and Singapore provides valuable lessons for China.
Hong Kong: The Forced Pivot
Hong Kong managed the elimination phase of the pandemic extremely well. A strategy based upon test trace and isolate meant that by the time vaccines were rolled out, Hong Kong had a cumulative population mortality from Covid of 26 per million people. At that time a Hong Kong resident was 68x less likely to have died of Covid than a resident of the UK. However, by early 2022 Hong Kong had the highest mortality rate in the world. The high mortality rate in the fifth wave was a direct result of two factors:
-
- Failure to vaccinate the most vulnerable
- Overloading of the health system
Both factors were influenced by the politicization of the public health response, which failed to adapt to evolving evidence and generally ignored the advice of Hong Kong public health experts in favour of second-guessing what may have been perceived as politically acceptable to China[2].
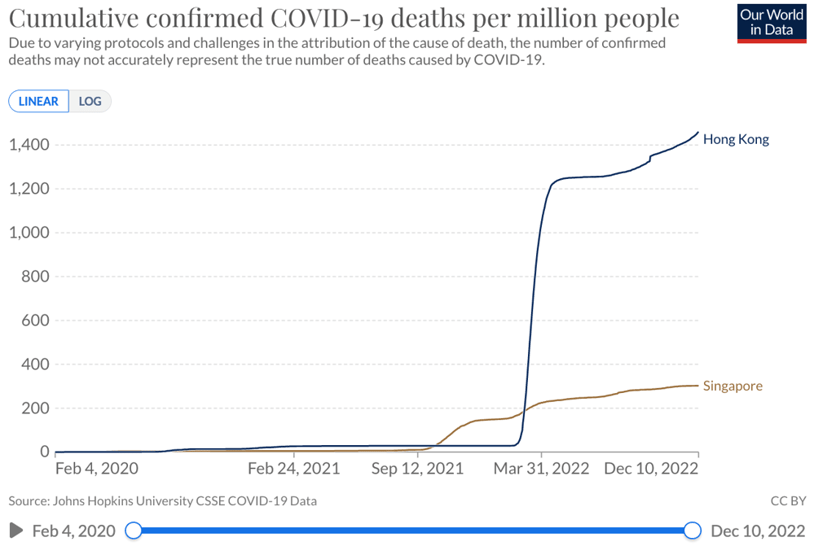
Fig 2. A graphic representation of the impact of the 5th wave in Hong Kong on cumulative population mortality. A result of 1) failing to vaccinate the vulnerable 2) Crashing of the health system.
Failure to Vaccinate the Vulnerable
Following a very successful first phase, the rollout of vaccines in Hong Kong was associated with mixed messaging played out against a background of low public trust. Although subsequent evidence from Hong Kong has shown killed vaccines to be effective after three doses, there was no evidence available at that time and unlike Singapore, Hong Kong ignored the international evidence in favour of mRNA vaccines. The withdrawal of available mRNA vaccines shortly after the vaccine program started, in addition to a focus on side effects and lack of clear messaging around benefits impacted confidence early.
Both messaging and policy in Hong Kong continued to focus on the strategy of elimination. Ignoring the single most important intervention, which was to increase vaccination levels for the vulnerable. The lack of a transitional plan resulted in a series of performative public health policies. Vaccine hesitancy in elderly Chinese is multifactorial and impacted by cultural factors including belief in Western medicines, fear of side effects of new vaccines, and perceptions of ageing, but the most important factor in low vaccine uptake in the vulnerable was a lack of perceived benefit[3]. The focus on the illusion of permanent zero Covid in addition to an exaggerated confidence in non-pharmacological interventions, especially masking, led to "rational" vaccine hesitancy.
‘In Hong Kong, the lack of any exit strategy resulted in a negative narrative focused on ‘keeping the bad guy out’. This created a climate of fear and encouraged rational vaccine hesitancy. The narrative around control and containment led to poor prioritisation and allocation of resources. Public health policy decisions increasingly became performative rather than substantive with very little, if any, grounding in science or evidence’
By mid-2021 it was obvious that whilst vaccinations are extremely effective at saving lives and reducing severe disease, they are less effective at preventing transmission. This meant that it would be impossible to achieve herd immunity by vaccination alone. The failure to accept, explain and adapt to the science resulted in Hong Kong having higher vaccination rates in ages 3-11 years than in ages 80+ despite the low vaccination in the elderly being the greatest threat to both the population and the health system. When the Omicron wave hit almost one year after the vaccines first became available, only 23% of those over 80 were fully vaccinated.
Overloading of the Health System
The fifth wave had a devastating impact on Hong Kong. The health system was overloaded leading to thousands of unnecessary deaths. Although the failure to vaccinate the vulnerable increased the pressure on hospitals other factors played a significant role in the breakdown of the health system. Under zero Covid, many asymptomatic or mildly symptomatic patients were kept in hospital under isolation, not for medical treatment but to prevent the spread of infections. The failure to plan an ordered transition meant that the hospital system was already at a high capacity when the fifth wave hit. A number of poor policy decisions aggravated this process. Compulsory testing notices began to overload capacity and people waited in line for long periods of time, often in the cold over the winter, to undertake these tests. Furthermore, health officials advised individuals with positive tests or symptoms to attend hospital and, later when the hospitals became overloaded, visit family clinics, many of which are in busy commercial buildings. All these decisions acted as accelerants in increasing community spread and subsequently stressing the hospital system. Predominantly elderly patients, but also those with disabilities, who tested positive were transferred from residential care homes into hospitals regardless of clinical need. The impact of the volume of cases over a short time overloaded the hospital system. Many of the deaths during this phase were not caused directly by Covid. Patients were not adequately hydrated nor given oxygen or other basic medications. Many did not have beds within the hospital and were treated in corridors or in the emergency department. It is well-recognized that all-cause mortality increases significantly when hospital systems break down. Emergency services were working above capacity and provision for other medical conditions was effectively suspended in some cases for months. We are yet to fully appreciate the impact on excess mortality of a focus on zero Covid in Hong Kong.
In summary, the lack of a backup transitional plan meant that Hong Kong delayed the inevitable pivot until it was too late. The focus on case identification rather than transition to disease management significantly increased mortality. The emphasis on politics over science and the focus on case numbers rather than disease is still driving irrational policies in Hong Kong which, along with false statements from health officials, continues to damage trust in Hong Kong health institutions. One example of disinformation is the suggestion that the fifth wave was triggered by the Cathay Pacific flight crew. The crew, who have recently been jailed, did trigger a small cluster of BA.1 infections. However, the huge BA.2 wave was triggered by transfer within 21-day hotel quarantine, a non-evidence-based policy which had already resulted in several 'near misses'.
‘There is no scientific evidence to support 21-day quarantine. It is neither evidence-based nor proportionate and is almost certainly doing more harm than good.’
- Is Hong Kong’s 21-day quarantine evidence based or justified: October 2021
Singapore: The Planned Pivot
All countries struggled at different stages of the pandemic and Singapore was no exception. Early cases in overseas workers threatened to overwhelm the elimination capacity. However, Singapore developed capacity in testing, tracing and isolation and procured vaccines relatively early. On the basis of the best currently available evidence, the Singapore Health department prioritized mRNA vaccines, focused on early vaccination of the most vulnerable and developed a clear and well-communicated plan to transition from zero Covid. Overall Singapore adapted to evolving evidence and communicated effectively. This process was facilitated by high levels of population trust in the government.
It is important to appreciate that the transition in Singapore took place over 6 to 12 months. This involved a change in messaging to prepare the population. It also involved ongoing measures of mitigation. Examples of mitigation include masks, work from home, school closures etc. These non-pharmacological interventions were used to suppress the wave of infections and minimise pressure on the health system as the population gradually built up an immunity wall. In Singapore, this wall was prepared with high population levels of effective vaccination with naturally acquired immunity from infection filling in the blanks over a period of months.
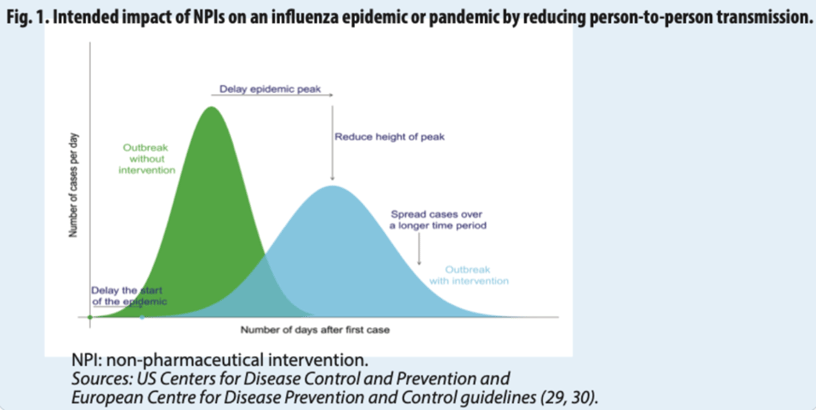
Fig 3. Non-pharmacological interventions (NPI’s) mitigate infective waves by spreading the infections over a longer period of time. The total number of infections is very similar but ‘flattening the wave’ protects the health system[4]
Singapore has now removed almost all Covid restrictions and economic activity and air travel have effectively returned to normal. Singapore has one of the lowest pro-rata Covid mortality rates in the world. Hong Kong continues to have restrictive social distancing policies whilst the economy continues to struggle. A resident of Hong Kong is almost 5x as likely to have died of Covid over the last 3 years than a resident of Singapore. This differential mortality rate is a reflection of two different strategies:
-
- Zero Covid with a planned exit = The best strategy
- Zero Covid with no transitional plan = A bad strategy
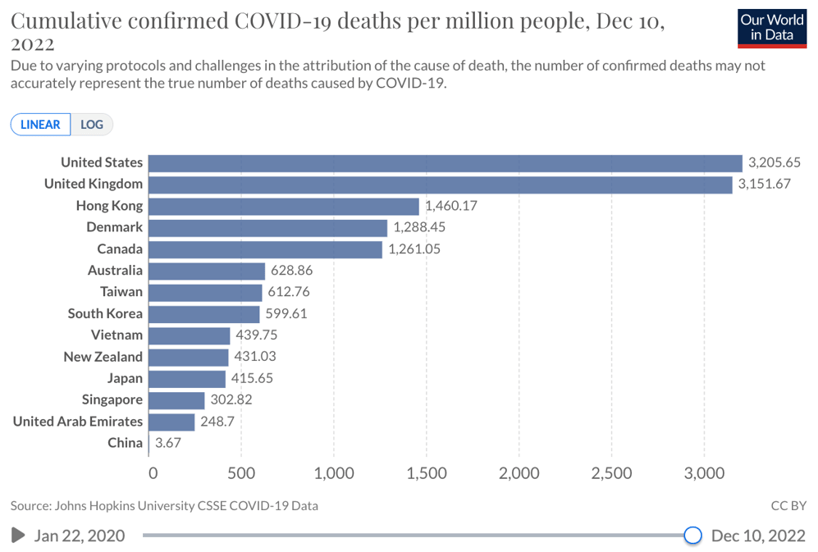
Fig 4. Hong Kong has overall mortality rates similar to the better-performing suppress and lift countries but 2-5X worse than the other elimination countries.
The Challenge to China of Evolving Variants and Pandemic Fatigue
Methods of containment invariably involve political decisions. Restriction of movement and quarantine are decisions which balance the rights of the individual against the rights of the majority. This process can be critiqued in philosophical and political terms. There have been criticisms internationally during Covid that public health interventions have been both slow and inadequate but also that they have been excessive. It is important to appreciate that control of infectious disease, by definition, has a significant political and economic component and the narratives around the management of infectious disease must be understood in this context. The traditional Western narrative around the China Covid response tends to focus on 'excessive restriction of individual rights’ and the ‘failure to import mRNA vaccines'. In reality, the elimination policy in China was successful at protecting the population in the first phase of the pandemic. There was a high level of public trust in this strategy. However, this has changed over the last few months. What has been driving this change?
Evolving Variants
Omicron variants have become increasingly transmissible spreading worldwide in waves within immune populations with a combination of waning immunity, both natural and vaccine-induced and immune escape (an increasing ability to dodge existing immunity). China has relatively low levels of population immunity. It has been obvious for some time that there have been increasing episodic clusters with a corresponding increase in the frequency, length and inconvenience of lockdowns, which along with other Covid policies, have had an increasingly negative impact on the economy. Recently China stopped tracing contacts of contacts. The implication being that the capacity had broken down at this level of tracing. Notwithstanding the political narrative of permanent zero Covid, it has been apparent that similar to Hong Kong in late 2021, the situation in China has been brittle for some time.
Pandemic Fatigue
Elimination policies in China and Hong Kong focused on population control. Mandatory PCR testing and quarantine were prioritised over education and trust in individuals. It is against this backdrop of central control that the challenge of the recent protests in China must be understood. The protests were ostensibly triggered by a fatal fire in Urumqi and aggravated by pictures of maskless fans at the football World Cup. In reality, stress has been building for some time. For those of us with lived experience, it seems hard to appreciate that there has been an academic debate as to whether pandemic fatigue is a real entity or a social construct. A recent review of pandemic fatigue[5] emphasised the importance of impact beyond the health domain. Over the study period, fatigue increased mistrust, protest and conspiracy beliefs, ‘fatigued people became frustrated activists, not submissive authoritarians’. Not surprisingly fatigue increases as mortality rates reduce. It is intuitively logical that people are less accepting of policies which have lower perceived benefits. Gaslighting and misinformation increase distrust and anger.
It is within this context of increasingly transmissible variants and rapidly increasing frustration with restrictive controls that China faced a dilemma. The science of both Covid and behavioural psychology would support a managed pivot but the current vaccination levels and population messaging are not yet optimal to transition to managed endemicity (living with covid). The suddenness and speed of the pivot in China suggests that the political calculation was such that the increasing difficulty and costs of elimination in addition to the risks associated with increasing fatigue were greater than the risks associated with a rapid transition.
What Lessons For China from Hong Kong and Singapore
China has recently announced a significant policy shift including an emphasis on vaccination for the vulnerable. Recent communication suggested that 76.6% of those over 80 in China have received 2 doses of Covid vaccine and 65.8 have had 3 doses. Most vaccines given in China are killed vaccines. Evidence from the BA.2 wave in Hong Kong suggests that providing individuals receive 3 doses, these vaccines are >98% effective against death and severe disease[6]. The narrative around mRNA vaccines is moot. Although mRNA vaccines are better at inducing an antibody response after two doses and have a higher impact on transmission, killed vaccines are good vaccines providing the vulnerable can receive 3 or 4 doses. The best vaccine in this context is the one that you can get into the arms of the vulnerable as quickly as possible.
Reports of PCR positivity in addition to anecdotal reports from Chinese cities suggest that the exit wave is already underway in China. It seems likely that China is in a similar situation to Hong Kong in early to mid-January 2022. By that point, Hong Kong had only fully vaccinated 23% of the most vulnerable and there was no shift in emphasis to boost vaccination throughout the first quarter of 2022. China already has better vaccination levels than Hong Kong but one clear lesson from Hong Kong would be to drive vaccinations and boosters as quickly as possible from the most vulnerable down even at this relatively late stage. A further lesson from Hong Kong is the importance of continuing mitigation during the transition period. Hong Kong was able to delay the doubling time of BA.2 from two days (seen internationally) to 3.1 days. It is likely that the impact in Hong Kong would have been even worse without the social distancing policies in place at that time.
Notwithstanding the benefit of mitigation policies, at the beginning of the fifth wave, Hong Kong continued the narrative and messaging of elimination. The pivot in messaging was far too late and this drove the overloading of the hospital system. It is clear that messaging in China is pivoting rapidly. Any shift in messaging has the potential to create confusion. For most of the last three years messaging in China has focused on the importance of keeping this dangerous virus under control. Now the narrative must shift to encouraging vaccination in the vulnerable whilst reassuring people that although this is a serious disease in some situations, for the majority it can be managed safely by isolating at home. It is essential that the hospital system is protected and this requires education and reassurance to individuals. It makes sense to transition to rapid tests rather than PCR and to clear the hospitals of anybody who does not need to be managed for clinical reasons. As many cases as possible should be managed in the community. In Hong Kong, the failure to act decisively, continuing to manage asymptomatic cases in hospitals and focusing on case identification rather than disease management crashed the hospital system resulting in thousands of unnecessary deaths. In this context the rapid pivot in communication within China makes sense.
In Hong Kong, the Covid wave peaked over January and February 2022. The mortality was back-end loaded with most deaths occurring in March and April 2022. Because of a combination of the geographic area and inherent policy controls, it may well be that China can mitigate and flatten the impending wave but it seems likely that mortality rates will begin to rise in China within the next couple of months meaning early action is critical. This action should focus on vaccination but it will also require ongoing mitigation, even the possibility of further lockdowns in order to spread the inevitable infections over a longer period of time to protect the health system. One of the most important lessons to be learned from Hong Kong is that omicron is not inherently milder in populations with no immunity. The size of the population means that regardless of mortality rates the absolute numbers will be large. If China exits with final mortality rates between those achieved in Singapore and Hong Kong it would mean a total mortality somewhere between 430 thousand and 2 million. We should all hope that by learning and reacting to lessons learned in Hong Kong and Singapore, China is able to exit with the smallest possible impact in population terms.
The key lesson from Singapore is that it is possible to transition from elimination to living with Covid but this requires high levels of vaccination from the most vulnerable down and a well-communicated transitional plan including ongoing mitigation during the transition phase. The lesson from Hong Kong is that failure to vaccinate the vulnerable and failure to acknowledge and positively communicate the need for such a plan can be devastating to population health.
Reference
1. Oliu-Barton, M., Pradelski, B. S. R., Aghion, P., Artus, P., Kickbusch, I., Lazarus, J. V., Sridhar, D., & Vanderslott, S. (2021, April 28). SARS-COV-2 elimination, not mitigation, creates best outcomes for health, the economy, and Civil Liberties. The Lancet. Retrieved December 13, 2022, from https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00978-8/fulltext
2. Julietwalker. (2021, August 20). Transitioning from covid-19 elimination to sustainable endemicity in East Asia. The BMJ. Retrieved December 13, 2022, from https://blogs.bmj.com/bmj/2021/08/11/transitioning-from-covid-19-elimination-to-sustainable-endemicity-in-east-asia/
3. Yuan, J., Lam, W. W. T., Xiao, J., Ni, M. Y., Cowling, B. J., & Liao, Q. (2022, June 16). Why do Chinese older adults in Hong Kong delay or refuse covid-19 vaccination? A qualitative study based on grounded theory. Why do Chinese older adults in Hong Kong delay or refuse COVID-19 vaccination? A qualitative study based on Grounded Theory. Retrieved December 13, 2022, from https://academic.oup.com/psychsocgerontology/advance-article/doi/10.1093/geronb/gbac184/6843313?login=false
4. World Health Organization. (n.d.). Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza. World Health Organization. Retrieved December 14, 2022, from https://www.who.int/publications-detail-redirect/non-pharmaceutical-public-health-measuresfor-mitigating-the-risk-and-impact-of-epidemic-and-pandemic-influenza
5. McMenamin, M. E., Nealon, J., Lin, Y., Wong, J. Y., Cheung, J. K., Lau, E. H. Y., Wu, P., Leung, G. M., & Cowling, B. J. (2022, January 1). Vaccine effectiveness of two and three doses of BNT162B2 and Coronavac against covid-19 in Hong Kong. medRxiv. Retrieved December 13, 2022, from https://www.medrxiv.org/content/10.1101/2022.03.22.22272769v2
6. Jørgensen F;Bor A;Rasmussen MS;Lindholt MF;Petersen MB; (n.d.). Pandemic fatigue fueled political discontent during the COVID-19 pandemic. Proceedings of the National Academy of Sciences of the United States of America. Retrieved December 13, 2022, from https://www.pnas.org/doi/10.1073/pnas.2201266119



